Authored by: Devin Zarkowsky MD
When asked by the surgery department chair as a medical student why I wanted to treat vascular patients, my response was to be useful, useful to people with a challenging systemic disease that often results in stroke, amputation, and death. Often, wounds that haven’t healed for months on a foot or a hand, or persistent leg pain provoked by walking or simply laying in bed are subtle indicators that Peripheral Arterial Disease (PAD), a vascular health challenge affecting many in our community, is present.
Allow me to relate one person’s recent medical journey. A gentleman in his 70’s was referred by his podiatrist. Wounds on his foot associated with a previous surgery had not healed for 5 months; his care team noted similar wounds at least 3 months prior to the surgery. Without his podiatrist recognizing poor wound healing as a sign of PAD, he could have lost his leg. Following a minimally-invasive procedure to restore blood flow below his ankle, his wound healed completely and he is alive on two legs, living a rewarding life surrounded by his children and grandchildren.
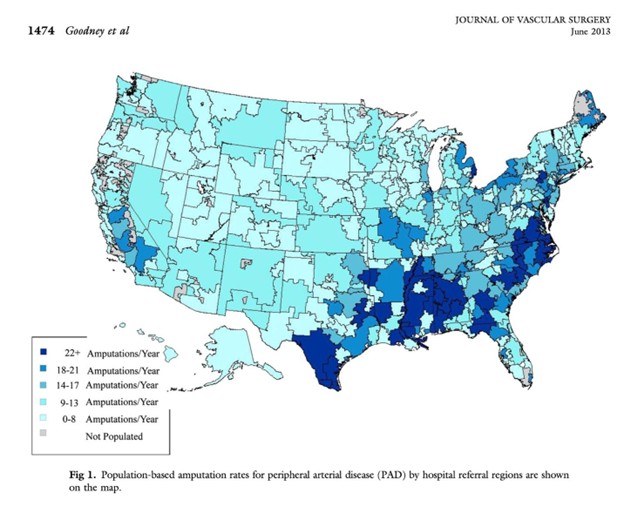
Writing is important to me and I’ve spent a good deal of my professional life learning to digest medical data and communicate the information in an approachable way; the adjacent pictures were published by a Philip Goodney MD, a Professor of vascular surgery at Dartmouth-Hitchcock Hospital in New Hampshire and a mentor of mine. They demonstrate amputation rates across the United States relative to population density. Notice Fallbrook is adjacent to the darker blue region in Southern California, meaning there is an unmet need and people right here are suffering relatively more amputations related to PAD than other US regions. Around the world, more than 200 million people have PAD; PAD patients are in good company and there is work to do for all of them.
Knowing this, and that at my core I want to be useful, it seems important to ensure PAD awareness is a local effort. Treating this disease process effectively often requires regular visits with your vascular surgeon, which I’ve learned over time can tax patients with mobility challenges. The closer doctors can be geographically to patients, the easier it is for us to overcome this health challenge together.
Nowadays, PAD care happens in the office setting rather than at a hospital. Portable ultrasounds, mobile X-ray equipment, as well as minimally invasive devices allow blocked arteries to be diagnosed and reopened under local anesthetic. Selected complex patients may still require hospital care, but most folks can be treated from start to finish without leaving town.
When PAD patients – or anyone with a medical condition – travel outside of their hometown area, it is important to check health insurance parameters – some plans restrict where care may be administered. Keep in mind that the most flexible and portable insurance coverage is Medicare Part B. Those eligible for Medicare Part B may visit any hospital in the US and just about any specialist doctor they choose. Insurance open enrollment happens every year in the Fall, providing an opportunity to select the right coverage. Folks should be aware that the freedom to receive care from their doctors is an important feature provided by Medicare Part B. Counseling is available at my office, California Vascular Health Specialists, through a host of resources during this open enrollment period, should anyone with PAD or another health condition have questions about signing up for Medicare Part B or the related supplements, Parts G, K, and L.
Our gentleman with the foot wound for months, was not able to access care locally and travelled a significant distance to my office. Adding a geographic barrier to his language barrier nearly lead to an amputation – an outcome suffered by up to 25% of PAD patients with this most severe form of the disease chronic limb-threatening ischemia or CLTI – all related to the economic challenge of maintaining a stable medical community in our corner of Southern California.
As a physician, I’ve learned that health care isn’t just about medicine. It’s about proximity. It’s about relationships. And sometimes, it’s about whether help is fifteen minutes away—or an hour and a half.
I practice vascular surgery in Fallbrook, California, a community on the northern edge of San Diego County. It’s not isolated, but it’s not urban either. People here value independence. They don’t want to leave town for every doctor’s visit, and many simply can’t. Over the years, I’ve watched what happens when local medical care quietly erodes. The consequences are not theoretical. They show up in exam rooms, wheelchairs, and nursing facilities.
This is not just a rural problem. It’s a community problem. Across the country, independent medical practices—often the backbone of care for working-class, elderly, and underserved patients—are disappearing. Over the last decade, the share of physicians in independent practice has dropped dramatically. When those practices close, patients drive farther, pay more, and often receive care in higher-cost hospital settings that were never meant to replace local medicine.
A major driver of this trend is how Medicare pays physicians. The Medicare Physician Fee Schedule (MPFS) was created to pay doctors for their work—their expertise, judgment, and time. As medical technology has advanced and more minimally invasive care can be provided safely in the office-based setting, patients have benefited greatly from better access to care and lower costs. However, as the MPFS was not built to reimburse for high-tech, high-cost equipment, the reimbursement schedule has been diluted and broken down for all physicians providing care in the office-based setting. The result? In hundreds of cases, reimbursement doesn’t even cover the basic cost of providing care, forcing practices to close or sell to large hospital systems.
The 2026 MPFS represented the first increase for office-based care in years, but permanent stability will require structural reform: specifically, paying separately from the MPFS for equipment and supplies, just as we already do in hospital and surgical center settings. That change would help keep doors open in communities where patients live.
Insurance coverage does not equal access to care. Communities need doctors nearby—doctors who know their patients, their histories, and their lives. My goal is simple: to keep my doors open so the next patient with a small problem doesn’t lose something irreplaceable.