

Introduction
Despite billions of dollars invested in digital health innovation, one of healthcare’s most fundamental processes, the patient referral, remains predominantly manual, fragmented, and prone to failure. Whether a hospital discharge planner is seeking post-acute care placement or a primary care physician is referring to a specialist, the typical referral journey still relies heavily on telephone calls, fax machines, and spreadsheet tracking systems.
This archaic approach generates staggering costs and poor outcomes. Healthcare systems lose an estimated $150 billion annually to referral leakage, with individual physicians accounting for $821,000 to $971,000 in annual revenue loss (DialogHealth, 2025). Only 34.8% of referral attempts result in documented completed appointments in large health systems (Patel et al., 2018). The patient referral management software market is experiencing explosive growth, reflecting urgent demand for solutions to these persistent challenges (Precedence Research, 2025).
This article examines the root causes of referral failures and explores how artificial intelligence-driven systems can deliver intelligent, privacy-preserving solutions to this persistent healthcare challenge.
The Anatomy of a $150 Billion Problem
Healthcare referrals suffer from interconnected inefficiencies creating massive financial losses and patient safety risks. Cross-institutional referrals face particularly acute challenges, with physicians reporting excessive faxed documents, missing or delayed documentation, and organisational privacy policies interfering with information exchange (Savoy et al., 2023). Research across 34 countries demonstrates that communication breakdowns between general practitioners and specialists remain a persistent global issue, resulting in fragmented care and compromised quality (Scaioli et al., 2020).
A comprehensive analysis of 103,737 referral attempts revealed that only 34.8% resulted in documented completed appointments (Patel et al., 2018). Hospital length-of-stay for patients awaiting post-acute care placement increased 24% from 2019 to 2022, with this increase persisting even after accounting for higher patient acuity (American Hospital Association, 2022). This discharge delay crisis manifests nationally: in Massachusetts, nearly one in seven non-ICU beds are occupied by patients medically ready for discharge, whilst in Nebraska, more than 100 patients waited over 30 days for post-acute care placements (ATI Advisory, 2024).
The financial impact is staggering. Healthcare systems lose between $200-500 million annually to referral leakage, with each physician’s out-of-network referrals translating to $821,000-$971,000 in annual revenue loss (DialogHealth, 2025). Nationally, referral leakage costs U.S. hospital systems an estimated $150 billion annually. The operational burden compounds these losses: discharge planners report making 10-15 phone calls over 3-10 days to secure each patient placement, whilst approximately 19.7 million clinically inappropriate referrals occur annually because providers lack reliable specialist information (DialogHealth, 2025).
Why Traditional Solutions Have Failed
Electronic health record systems have digitised documentation but largely failed to solve referral coordination. A study found nearly half of external referrals still arrived via fax despite available EHR-based electronic referral functionality (Hughes et al., 2020). Recent systematic reviews examining interventions from 2018-2024 confirm that whilst structured referral proformas and educational interventions show promise, implementation success remains highly context-dependent (Saghdaoui et al., 2025).
The problem stems from fragmentation and lack of standardisation. Referral criteria differ by insurance payer, care setting, specialty, and region. A 2020 study examining family medicine practices found average monthly referral rates of 20.3%, with significant variation between clinic groups, highlighting inconsistent referral patterns across similar practice settings (El Ayadi et al., 2021). Research indicates that whilst physicians require detailed specialist information for effective referrals, significant gaps persist in access to this critical data (PerfectServe, 2024).
From patients’ perspectives, limited health literacy, transportation challenges, and difficulty navigating complex systems compound breakdowns. Cross-institutional referrals result in increased staff burden, patient frustration, and delays in diagnosis compared to internal referrals (Savoy et al., 2023). Without tools to track referral status or receive guidance, patients frequently become lost in the system, with completion rates remaining disappointingly low across various healthcare settings.
Engineering Intelligent Solutions: AI-Powered Referral Coordination
Modern referral solutions must transcend digitisation to deliver intelligent automation addressing the multi-dimensional nature of this challenge. Advanced systems employ several key architectural components grounded in recent research findings.
Graph-based modelling represents the healthcare ecosystem as a dynamic structure where nodes represent patients, facilities, providers, and services, whilst edges represent care relationships and eligibility constraints. Analysis of the U.S. Patient Referral Network spanning 2009-2015 reveals power law distributions and core-periphery structures at both state and national levels, with certain physicians serving as hubs for patient-sharing relationships (An et al., 2018). AI algorithms can traverse this complex graph in real-time to identify optimal matches based on multiple simultaneous constraints.
Multi-constraint satisfaction enables screening based on specific care needs, location, insurance acceptance, real-time capacity, specialised equipment, and patient preferences, all whilst using minimal, de-identified data during matching. This addresses critical gaps in current systems where providers lack access to essential specialist information needed for appropriate referral decisions (DialogHealth, 2025).
Privacy-preserving architectures implement ephemeral communication patterns where sensitive information is shared via encrypted, time-limited channels with no persistent intermediary storage. This maintains HIPAA compliance whilst enabling efficient information flow, addressing the security vulnerabilities and privacy concerns identified in cross-institutional referral studies (Savoy et al., 2023).
Automated workflow coordination augments rather than replaces human judgement, handling routine tasks like identifying eligible facilities, checking availability, routing requests, tracking status, and coordinating logistics. This allows coordinators to focus expertise on complex cases whilst systems handle routine coordination. High-performing organisations achieve referral completion rates of 85-95% through systematic approaches to referral management (HealthViewX, 2025).
From Personal Experience to Healthcare Innovation: The Carenector Story
Carenector exemplifies how personal healthcare challenges can catalyse systematic solutions. The platform emerged from the convergence of two complementary perspectives: a PhD student who struggled to find physical therapy following ACL reconstruction surgery that was both accessible and accepted his insurance, and a Director of Social Work at a leading nursing facility who managed the daily tedious work of discharge planning and finding appropriate post-acute care placements for patients.
These co-founders recognised their individual frustrations represented systemic failures affecting millions. The PhD student’s experience revealed patient-facing gaps: lack of transparent information about facility locations, insurance acceptance, and availability; difficulty comparing options across multiple criteria; and absence of streamlined search tools. The social worker’s professional experience highlighted provider challenges documented in research: spending 10-15 calls and 3-10 days per placement; managing referrals through manual spreadsheets, faxes, and phone calls; losing track of status across concurrent cases; and lacking visibility into facility capacity.
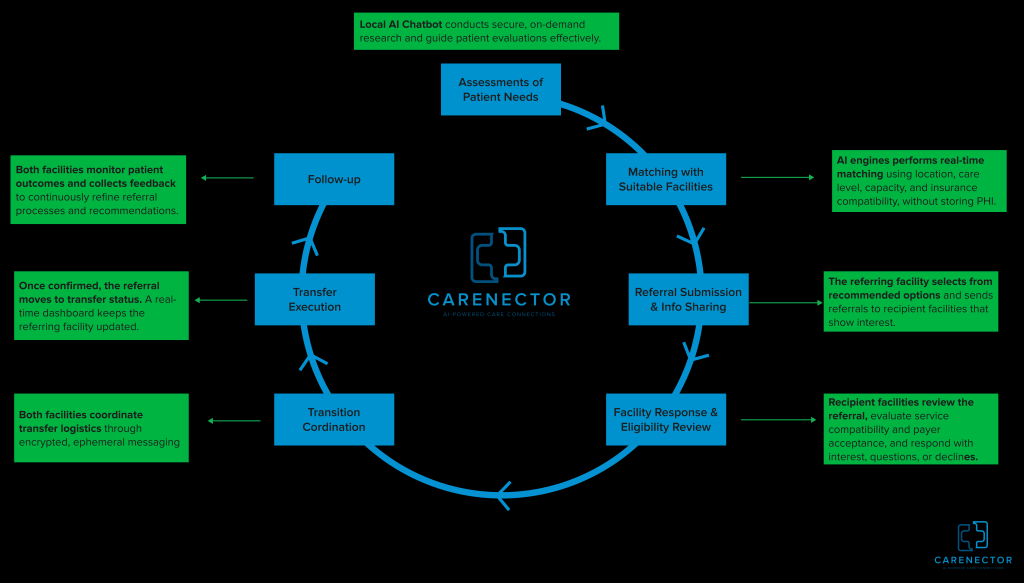
The platform they developed addresses both sides. For individuals and families, Carenector enables searches based on ZIP code, insurance, and care needs without upfront disclosure of sensitive health information, providing transparent results with real-time availability. For healthcare facilities, the system employs real-time matching across multiple dimensions: care level, geographic proximity, insurance compatibility, current capacity, and quality metrics.
Structured intake prompts eliminate ambiguity from unstructured communications identified as major barriers in recent research (Savoy et al., 2023). Expiring secure links enable HIPAA-compliant information sharing. Unified dashboards provide status tracking without platform switching, addressing the communication breakdowns documented across international healthcare systems (Scaioli et al., 2020). Optional outcome feedback enables continuous algorithm improvement, working towards the 85-95% completion rates achieved by high-performing organisations (HealthViewX, 2025).
Beyond Technology: Requirements for Transformation
Resolving the referral crisis requires more than technology, it demands comprehensive workflow reengineering and policy support. Recent systematic reviews emphasise that successful interventions depend on specific clinical contexts and implementation practicalities (Saghdaoui et al., 2025). Solutions must be grounded in actual workflows of discharge planners, nurses, case managers, and social workers managing daily referrals.
Standards adoption is essential. Embracing HL7 FHIR for data exchange and SNOMED CT for clinical terminology ensures platforms communicate effectively across diverse EHR systems. Given that healthcare organisations continue struggling with EHR-based referral functionality despite its availability (Hughes et al., 2020), standards-based integration becomes critical. The shift towards cloud-based and web-based referral platforms demonstrates the industry’s movement towards more interoperable solutions.
Change management requires genuine frontline buy-in. Research demonstrates significant physician resistance to modifying referral patterns without support and clear benefits (DialogHealth, 2025), underscoring the importance of effective change management strategies. Policy interventions such as CMS reimbursement for referral tracking, quality metrics measuring completion rates, and mandates for electronic infrastructure, could accelerate adoption. The American Hospital Association’s 2022 call for temporary per diem Medicare payments to address discharge delays reflects growing policy recognition of this crisis (American Hospital Association, 2022).
Patient engagement through transparent platforms improves completion rates by providing status visibility, clear instructions, reminders, and educational resources. Cross-institutional studies reveal that current systems create increased patient frustration and delays in diagnosis (Savoy et al., 2023), highlighting opportunities for improvement through better patient-facing tools. Rigorous evaluation measuring completion rates, timeliness, appropriateness, and clinical outcomes accelerates field-wide learning.
The Path Forward
Referrals span virtually every specialty and patient population. Improving this fundamental process is essential for value-based care, population health management, and health equity. The patient referral management software market’s substantial growth reflects urgent demand for solutions to these persistent challenges.
The transformation is far from complete, but technological capabilities exist today to dramatically improve referral processes. Research-driven innovations like Carenector, born from lived experiences of navigating post-surgical care and managing daily discharge challenges, demonstrate that well-designed AI systems can address real-world coordination challenges whilst respecting privacy and regulatory requirements.
The need has never been more urgent. As healthcare faces mounting pressures, ageing populations requiring complex coordination with hospital length-of-stay up 24% for post-acute discharges (American Hospital Association, 2022), only 34.8% of referral attempts resulting in documented completed appointments (Patel et al., 2018), and systems hemorrhaging $150 billion annually to leakage (DialogHealth, 2025), intelligent automation transitions from efficiency gain to fundamental necessity for sustainable healthcare delivery. The tools are available. The evidence is compelling. The time for transformation is now.
References
- Bolton Saghdaoui, L., Lampridou, S., Tavares, S., Lear, R., Davies, A. H., Wells, M., & Onida, S. (2025). Interventions to improve referrals from primary care to outpatient specialist services for chronic conditions: a systematic review and framework synthesis update. Systematic Reviews, 14(1), 103.
- American Hospital Association. (2022). Issue brief: Patients and providers faced with increasing delays in timely discharges. https://www.aha.org/issue-brief/2022-12-05-patients-and-providers-faced-increasing-delays-timely-discharges
- ATI Advisory. (2024). The hospital discharge crisis: Defining the challenge. https://atiadvisory.com/resources/the-hospital-discharge-crisis-defining-the-challenge-2/
- Savoy, A., Khazvand, S., Mathew, A., Gilmore, A. M., Cottingham, E., Sangani, A., … & Damush, T. M. (2023). Consultants’ and referrers’ perceived barriers to closing the cross-institutional referral loop, and perceived impact on clinical care. International journal of medical informatics, 180, 105265. DialogHealth. (2025). 30+ patient referral statistics: Why your system is bleeding money. https://www.dialoghealth.com/post/patient-referral-statistics
- Patel, M. P., Schettini, P., O’Leary, C. P., Bosworth, H. B., Anderson, J. B., & Shah, K. P. (2018). Closing the referral loop: an analysis of primary care referrals to specialists in a large health system. Journal of general internal medicine, 33(5), 715-721.
- HealthViewX. (2025). Measuring success: Key performance indicators for referral management programs. https://www.healthviewx.com/measuring-success-key-performance-indicators-for-referral-management-programs/
- El Ayadi, H., Desai, A., Jones, R. E., Mercado, E., Williams, M., Rooks, B., & Carek, P. J. (2021). Referral rates vary widely between family medicine practices. The Journal of the American Board of Family Medicine, 34(6), 1183-1188.
- An, C., O’Malley, A. J., Rockmore, D. N., & Stock, C. D. (2018). Analysis of the US patient referral network. Statistics in medicine, 37(5), 847-866.
- PerfectServe. (2024). Prevent patient leakage with in-network referrals. https://www.perfectserve.com/blog/patient-leakage/
- Precedence Research. (2025). Patient referral management software market size to hit USD 67.92 billion by 2034. https://www.precedenceresearch.com/patient-referral-management-software-market
- Scaioli, G., Schäfer, W. L. A., Boerma, W. G. W., Spreeuwenberg, P. M. M., Schellevis, F. G., & Groenewegen, P. P. (2020). Communication between general practitioners and medical specialists in the referral process: A cross-sectional survey in 34 countries. BMC Family Practice, 21(1), 54. https://doi.org/10.1186/s12875-020-01124-x
- Hughes, C. A., Allen, P., & Bentley, M. (2018). eReferrals: Why are we still faxing?. Australian journal of general practice, 47(1/2), 51-56.
- Carenector (2025): https://carenectorhealth.com/
